
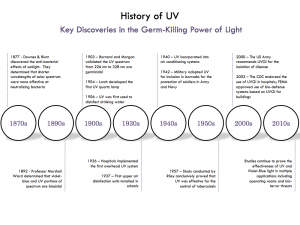
“UVC lamps on the ceilings at an airport”
REAL WORLD TESTING
https://nature.com/articles/s41598-022-08462-z
http://star.st-and.ac.uk/~kw25/research/UVC/UVC.html
https://physicsworld.com/potential-of-far-ultraviolet-light-for-pandemic
https://physicsworld.com/a/far-uvc-light-zaps-airborne-pathogens
Far-UVC light zaps airborne pathogens in realistic conditions
by Isabelle Dumé / 03 May 2022
“Far ultraviolet-C light can reduce the level of airborne microbes in a room by more than 92%, according to a new study by researchers in the UK and the US. The result suggests that lamps operating at this wavelength could be used to combat common airborne viruses, including SARS-CoV-2, and thus prevent the transmission of diseases like COVID-19. While ordinary UVC light is very effective at destroying microbes like bacteria and viruses, it is hazardous for humans because it can damage skin and eyes. A decade ago, researchers at Columbia University in the US discovered that a different wavelength of UVC light, known as far-UVC light, would be just as effective at killing germs, but without the safety concerns. This is because, at 222 nm, its wavelength is too short to penetrate human skin or eye cells. These early tests of the technology were, however, conducted in small experimental chambers, rather than room-sized ones that better reflect real-world human environments.
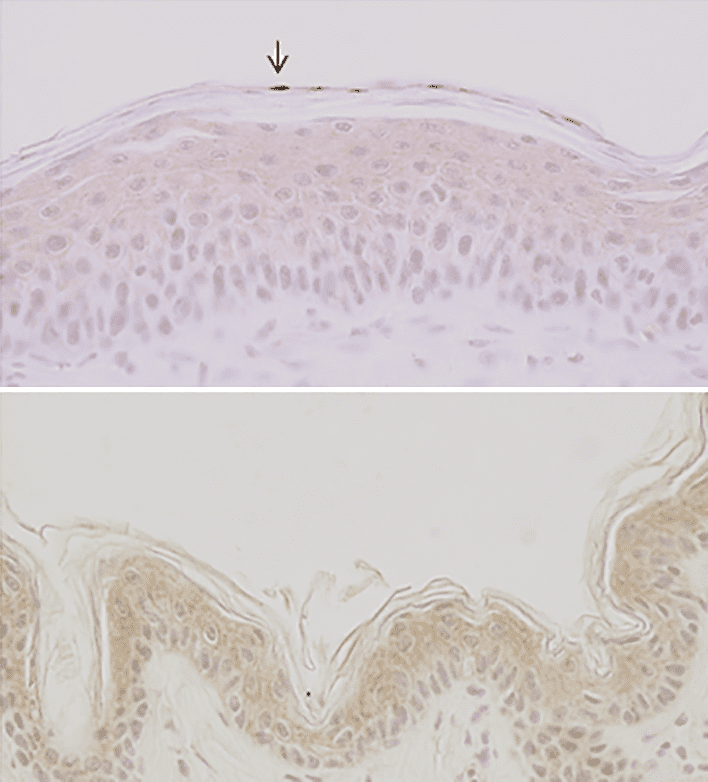
“A 32 nm difference: Mouse skin after irradiation with 254 nm UV light (top) shows DNA damage (marked by arrow). Mouse skin irradiated at 222 nm (bottom) does not show these lesions. (CC BY 4.0/PLOS One)”
In the new work, scientists from the universities of St Andrews and Leeds in the UK and Columbia University Vagelos College of Physicians and Surgeons tested the efficiency of far-UVC krypton chloride (KCl) excimer lamps in a specially designed room-sized chamber at Leeds. The researchers ventilated this chamber at the same rate as a typical home or office – that is, around three air changes per hour. They then released aerolized S. aureus bacteria into the space continuously, allowing the pathogen load to reach a stable level before sampling the air for an hour. While continuing to release the aerolized S. aureus into the chamber, the researchers then switched on the far-UVC lamps placed on the ceiling of the chamber and sampled the air for a further hour. “This methodology allowed us to compare the air samples after the lamps had been switched on compared to the air samples before lamp switch-on,” explains team member Kenneth Wood, a researcher in the School of Physics and Astronomy at St Andrews. The team found that the lamps reduced the continuously produced aerolized S. Aureus pathogen load in the room by 92%, which is equivalent to 35 air changes per hour. “This is exciting,” Wood tells Physics World, “since this is a higher number of air changes per hour than other technologies (which have been limited to 5 to 20 equivalent air changes).
It is also the first time the effect of far-UVC has been demonstrated for aerolized pathogens in a large ‘real-world’ type environment.” Wood adds that the trials have produced “spectacular results”, far exceeding what is possible with ventilation alone. “In terms of preventing airborne disease transmission, far-UVC light could make indoor places as safe as being outside on the golf course on a breezy day at St Andrews,” he says. Team member David Brenner, who leads the Center for Radiological Research at Columbia, says that far UVC-light should be just as good at inactivating current and future variants of SARS-CoV-2; new infectious viruses that have yet to emerge; and “old-fashioned” viruses like influenza and measles. The researchers foresee that far-UVC could become an important “hands off” tool, alongside filtration and ventilation, in a global move towards reducing airborne transmission of disease and improving indoor air quality. The team have received funding from NHS Scotland Assure to investigate the impact of far-UVC when there are different mechanical ventilation rates. “With this funding, we also plan to study how far-UVC acts on other pathogens and hopefully short-distance viral inactivation,” Wood says. The researchers would now also like to test the technology in real-world environments. The research is detailed in Scientific Reports.”
Could a new ultraviolet technology fight the spread of #coronavirus? “Far-UVC light has the potential to be a ‘game changer,’ ” said David Brenner, director of @Columbia’s Center for Radiological Research. https://t.co/lLR0RlnmDC pic.twitter.com/4ce9kKB8q0
— Columbia Vagelos College of Physicians & Surgeons (@ColumbiaPS) April 23, 2020
FAR-UVC LIGHT
https://ushio.com/product/care222-mercury-free-far-uv-c-excimer/
https://sterilray.com/excimer-wave-sterilray-luminaire/
https://ncbi.nlm.nih.gov/pubmed/30096188
https://ncbi.nlm.nih.gov/pubmed/24067444
https://ncbi.nlm.nih.gov/pmc/articles/PMC5552051
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0201259
https://kobe-u.ac.jp/research_at_kobe_en/NEWS/collaborations/2020_04_07_01.html
https://projectreporter.nih.gov/project_info_description.cfm?aid=9140848&icde=37994559
https://nature.com/articles/s41598-018-21058-w
New tool to control spread of airborne-mediated microbial diseases
February 2018
“Airborne-mediated microbial diseases such as influenza and tuberculosis represent major public health challenges. A direct approach to prevent airborne transmission is inactivation of airborne pathogens, and the airborne antimicrobial potential of UVC ultraviolet light has long been established; however, its widespread use in public settings is limited because conventional UVC light sources are both carcinogenic and cataractogenic.
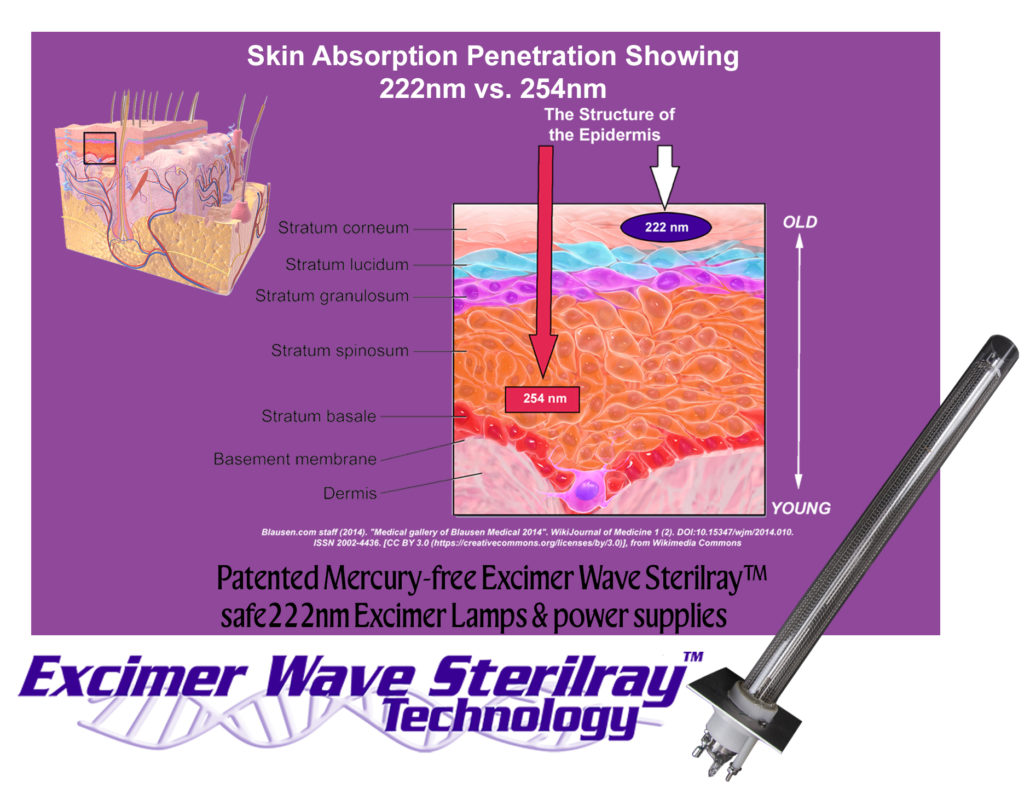
By contrast, we have previously shown that far-UVC light (207–222 nm) efficiently inactivates bacteria without harm to exposed mammalian skin. This is because, due to its strong absorbance in biological materials, far-UVC light cannot penetrate even the outer (non living) layers of human skin or eye; however, because bacteria and viruses are of micrometer or smaller dimensions, far-UVC can penetrate and inactivate them.

“A small ultraviolet lamp which emits what’s called far-UVC light would be effective in large public spaces such as airports as well as the close confines of airplane cabins.” (Columbia University Center for Radiological Research)
We show for the first time that far-UVC efficiently inactivates airborne aerosolized viruses, with a very low dose of 2 mJ/cm2 of 222-nm light inactivating >95% of aerosolized H1N1 influenza virus. Continuous very low dose-rate far-UVC light in indoor public locations is a promising, safe and inexpensive tool to reduce the spread of airborne-mediated microbial diseases.”
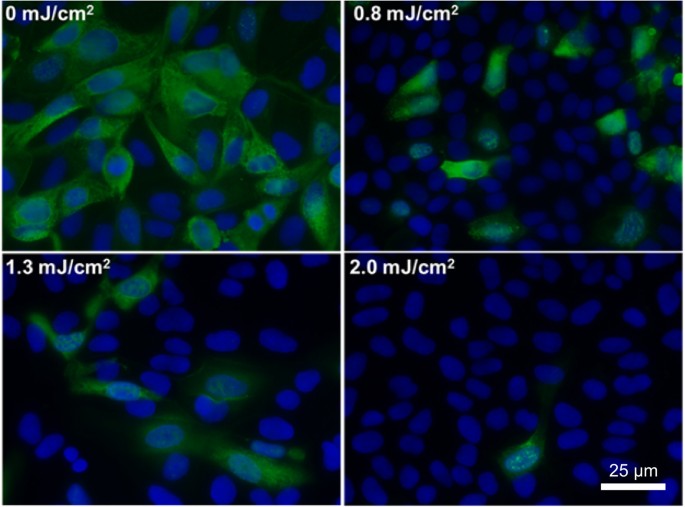
“Antiviral efficacy of different low doses of 222-nm far-UVC light.”
DON’T TRY THIS at HOME
http://iuva.org/iuva-covid-19-faq
http://iuva.org/IUVA-Fact-Sheet-on-UV-Disinfection-for-COVID-19
http://iuva.org/uv-light-on-human-body
UV Industry Associations Discourage Use of UV Light on the Human Body to Disinfect Against Coronvirus
by Gary Cohen / 24 Apr 2020
“Recent reports suggest that ultraviolet (UV) light can be used on the human body to disinfect against the coronavirus. The International Ultraviolet Association (IUVA) and RadTech North America are educational and advocacy organizations consisting of UV equipment vendors, scientists, engineers, consultants, and members of the medical profession.

We would like to inform the public that there are no protocols to advise or to permit the safe use of UV light directly on the human body at the wavelengths and exposures proven to efficiently kill viruses such as SARS-CoV-2. UV light under the conditions known to kill such viruses are also known to cause severe skin burns, skin cancer, and eye damage.
We strongly recommend that anyone using UV light to disinfect medical equipment, surfaces, or air in the context of COVID-19, applications that are supported by sound scientific evidence, follow all recommended health and safety precautions and to avoid direct exposure of the body to the UV light.
The ultraviolet spectrum is a band of electromagnetic radiation at higher energies than visible light, split into four major categories: UV-A (400 – 315 nm), UV-B (315 – 280 nm), UV-C (280 – 200 nm), and vacuum-UV (VUV, 100 – 200 nm).
UV-A and UV-B are present in sunlight at the earth’s surface; these parts of the ultraviolet spectrum are common causes of sunburn and, with longer-term exposure, melanoma. The risks of human exposure to UV-A and UV-B are well known. Solar UV may be used for disinfection purposes; exposures in the order of several hours to days might be effective at treating surfaces and water. Artificial sources of UV-A and UV-B are not commonly used for disinfection.
UV-C has been used for disinfection for over a century, with applications in water treatment, air systems, and surfaces. The use of UV-C as a disinfectant is supported by decades of scientific research. UV-C radiation is absorbed by DNA and RNA (the genetic code for all lifeforms), changing its structure. This damage inhibits the ability of the affected cells to reproduce, meaning that they cannot infect and are no longer dangerous. Whereas the UV exposure required to inactivate different microorganisms varies, though there are no known microorganisms that are immune to this treatment and it is regularly used against bacteria, viruses, and protozoa.
In the same way that UV-C can inactivate bacteria and viruses, it can be damaging to human cells too, since our cells also contain DNA. This exposure can cause skin irritation, damage to the cornea, and cell mutations leading to cancer. Exposure to UV-C radiation is regulated globally, with a common agreement on the risk to human health and safe exposure levels. These regulations and standards set limits on allowable exposure, though in all cases it is recommended to avoid UV exposure where possible.”
GERMICIDAL ULTRAVIOLET (GUV)
https://purolighting.com/technology
https://violetdefense.com/effectiveness-of-uv
https://crowdfund.columbia.edu/pages/cuimc-research
https://cdn2.hubspot.net/hubfs/455757/IES%20UV%20report.pdf
https://cuimc.columbia.edu/news/can-uv-light-fight-spread-influenza
https://link.springer.com/content/pdf/bfm%3A978-3-642-01999-9%2F1.pdf
https://crr.columbia.edu/using-power-light-preventing-airborne-coronavirus
https://columbia.edu/ultraviolet-technology-virus-covid-19-UV-light
Far-UVC light—safe for humans, but lethal for viruses
by Carla Cantor / April 21, 2020
“A technique that zaps airborne viruses with a narrow-wavelength band of UV light shows promise for curtailing the person-to-person spread of COVID-19 in indoor public places.
The technology, developed by Columbia University’s Center for Radiological Research, uses lamps that emit continuous, low doses of a particular wavelength of ultraviolet light, known as far-UVC, which can kill viruses and bacteria without harming human skin, eyes and other tissues, as is the problem with conventional UV light.
“Far-UVC light has the potential to be a ‘game changer,’” said David Brenner, professor of radiation biophysics and director of the center. “It can be safely used in occupied public spaces, and it kills pathogens in the air before we can breathe them in.” The research team’s experiments have shown far-UVC effective in eradicating two types of airborne seasonal coronaviruses (the ones that cause coughs and colds).
The researchers are now testing the light against the SARS-CoV-2 virus in collaboration with Thomas Briese and W. Ian Lipkin of the Center for Infection and Immunity in a biosafety laboratory on Columbia’s medical center campus, with encouraging results, Brenner said.
The team previously found the method effective in inactivating the airborne H1N1 influenza virus, as well as drug-resistant bacteria. And multiple, long-term studies on animals and humans have confirmed that exposure to far-UVC does not cause damage to the skin or eyes.
If widely used in occupied public places, far-UVC technology has the potential to provide a powerful check on future epidemics and pandemics, Brenner said. He added that even when researchers develop a vaccine against the virus that causes COVID, it will not protect against the next novel virus. “Our system is a low-cost, safe solution to eradicating airborne viruses minutes after they’ve been breathed, coughed or sneezed into the air,” Brenner said.

“Not only does it have the potential to prevent the global spread of the virus that causes COVID-19, but also future novel viruses, as well as more familiar viruses like influenza and measles.” Brenner envisions the use of safe overhead far-UVC lamps in a wide range of indoor public spaces.

“NYC MTA demonstrates Puro UV-C technology inside a subway car”
The technology, which can be easily retrofitted into existing light fixtures, he said, could be deployed in hospitals and doctors’ offices as well as schools, shelters, airports, airplanes and other transportation hubs.
Scientists have known for decades that germicidal UV light (wavelength around 254 nm) has the capacity to kill viruses and bacteria. Hospitals and laboratories often use germicidal UV light to sterilize unoccupied rooms, as well as other equipment. But conventional germicidal UV light cannot be used in the presence of people as it can causes health problems to the skin and eyes.

In contrast, far-UVC light, which has a very short wavelength (in the range from about 205 to 230 nm), cannot reach or damage living human cells. But these wavelengths can still penetrate and kill very small viruses and bacteria floating in the air or on surfaces. Far-UVC lamps are now in production by several companies, although ramping up to large-scale production, as well as approval by the Food and Drug Administration and Environmental Protection Agency, will take several months.
At between $500 and $1000 per lamp, the lamps are relatively inexpensive, and once they are mass produced the prices would likely fall, Brenner said. “Far-UVC takes a fundamentally different tactic in the war against COVID-19,” Brenner said. “Most approaches focus on fighting the virus once it has gotten into the body. Far-UVC is one of the very few approaches that has the potential to prevent the spread of viruses before they enter the body.”
UVC STERILIZATION
https://royalsocietypublishing.org/doi/pdf/10.1098/rspl.1878.0109
https://blog.cleanslateuv.com/2018/10/evolution-of-uv-disinfection
http://www.uvresources.com/blog/uv-c-lamps-a-short-wave-history
https://insights.regencylighting.com/can-uv-light-kill-viruses-like-covid-19
https://uv-light.co.uk/safety-uv-light-industrial-medical-scientific-applications
https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-020-4847-9
https://techstartups.com/uv-light-kills-coronavirus-30-seconds-new-study
https://ul.com/news/ul-grants-purplesun-first-ever-mobile-uv-system-certification-large-scale-healthcare-equipment
https://bbc.com/future/article/20200327-can-you-kill-coronavirus-with-uv-light
Can you kill coronavirus with UV light?
by Zaria Gorvett / 24th April 2020
“You would literally be frying people,” says Dan Arnold, laughing in disbelief. Arnold works for UV Light Technology, a company that provides disinfecting equipment to hospitals, pharmaceutical companies and food manufacturers across the UK. Recently, as the global anxiety about Covid-19 has reached extraordinary new heights, he’s found himself fielding some unusual requests.
“We had an enquiry from a private individual about our equipment, saying ‘Well, why can’t we just get one of your UV lights and put it up on the exit to the supermarket – people can stand under it for a few seconds before they go in’,” he says.
Among the abundant “health” advice that has been swarming around the internet in recent weeks, the idea that you can disinfect your skin, clothing or other objects with UV light has proved extremely popular – and even been mentioned by the US President.
https://www.youtube.com/watch?v=WvsgyhGIeMA
So is this a good way to protect yourself from Covid-19? And is it true that since “the new coronavirus hates the sun”, sunshine will immediately kill it, as some reports on social media have claimed? In short: no. Here’s why. Sunlight contains three types of UV. First there is UVA, which makes up the vast majority of the ultraviolet radiation reaching the Earth’s surface.
It’s capable of penetrating deep into the skin and is thought to be responsible for up to 80% of skin ageing, from wrinkles to age spots. Next there’s UVB, which can damage the DNA in our skin, leading to sunburn and eventually skin cancer (recently scientists have discovered that UVA can also do this). Both are reasonably well known, and can be blocked out by most good sun creams.

There is also a third type: UVC. This relatively obscure part of the spectrum consists of a shorter, more energetic wavelength of light. It is particularly good at destroying genetic material – whether in humans or viral particles. Luckily, most of us are unlikely to have ever encountered any.
That’s because it’s filtered out by ozone in the atmosphere long before it reaches our fragile skin. Or that was the case, at least, until scientists discovered that they could harness UVC to kill microorganisms. Since the finding in 1878, artificially produced UVC has become a staple method of sterilisation – one used in hospitals, airplanes, offices, and factories every day.
Crucially, it’s also fundamental to the process of sanitising drinking water; some parasites are resistant to chemical disinfectants such as chlorine, so it provides a failsafe. Though there hasn’t been any research looking at how UVC affects Covid-19 specifically, studies have shown that it can be used against other coronaviruses, such as Sars. The radiation warps the structure of their genetic material and prevents the viral particles from making more copies of themselves.
However, it’s not quite as good as we might have hoped. In a recent study – which looked at whether UVC could be used to disinfect PPE – the authors found that, while it is possible to kill the virus this way, in one experiment it needed the highest exposure out of hundreds of viruses that have been looked at so far. The amount of ultraviolet required varied widely, depending on factors such as the shape and type of material the virus was on.
Nevertheless, a concentrated form of UVC is now on the front line in the fight against Covid-19. In China, whole buses are being lit up by the ghostly blue light each night, while squat, UVC-emitting robots have been cleaning floors in hospitals. Banks have even been using the light to disinfect their money.
At the same time, UV equipment suppliers have reported record sales, with many urgently stepping up production to fill their orders. Arnold says UV Light Technology has run out of all of its equipment already. But there’s a major caveat. “UVC is really nasty stuff – you shouldn’t be exposed to it,” says Arnold. “It can take hours to get sunburn from UVB, but with UVC it takes seconds.
If your eyes are exposed… you know that gritty feeling you get if you look at the sun? It’s like that times 10, just after a few seconds.” To use UVC safely, you need specialist equipment and training. The World Health Organization (WHO) has issued a stern warning against people using UV light to sterilise their hands or any other part of their skin.
During the White House briefing on Thursday, the US president suggested that UV light could be brought inside the body to kill the coronavirus. It’s not clear which type he meant, but given what we know about the damage UVA, UVB and UVC can do to genetic material and living tissues, this would be a bad idea – let alone impractical, since Covid-19 mostly infects the lungs.
Recently, scientists have discovered a promising new type of UVC which is less dangerous to handle, and still lethal to viruses and bacteria. Far-UVC has a shorter wavelength than regular UVC, and so far, experiments with human skin cells in the lab have shown that it doesn’t damage their DNA (more research is needed to be sure). On the other hand, bacteria and viruses don’t come off as well, because they are small enough for the light to reach.
One study found that it could prevent mouse wounds from becoming infected with the superbug MRSA, while another found that it could kill flu viruses suspended in the air. However, the vast majority of the UVC lamps on the market don’t use far-UVC yet – and again, it hasn’t been tested in actual humans, just on our cells in petri dishes and other animals. So this type of radiation probably won’t help you during the current pandemic either.
Would UVA or UVB work instead? And if so, does this mean you can disinfect things by leaving them out in the sun? The short answer: possibly – but you wouldn’t want to rely on it. In the developing world, sunlight is already a popular means of sterilising water – it’s even recommended by the World Health Organisation (WHO).
The technique involves pouring the water into a clear glass or plastic bottle, and leaving it out in the sun for six hours. It’s thought to work because the UVA in sunlight reacts with dissolved oxygen to produce unstable molecules such as hydrogen peroxide, the active ingredient in many household disinfectants, which can damage pathogens. Without water, sunlight will still help to disinfect surfaces – but it may take longer than you’d think.
The problem is we don’t know how long, because it’s still too soon for many studies to have been done on the new coronavirus. Just before President Trump’s comments about UV light on Thursday, William Bryan, a science and technology advisor at the Department of Homeland Security, presented some results from a study they have conducted into whether sunlight can kill the pathogen.
They found that when the virus was suspended in the air, its half-life – the amount of time it takes to deactivate half the particles in a particular sample – in “ordinary conditions” (20% humidity and a temperature of 70-75F (21.1-23.9C)) was around an hour.
When they added sunlight into the equation, that shrank to just one and a half minutes. However, the study results have so far only been alluded to in the briefing and a leaked report – they have not been officially published or peer-reviewed. It’s also not clear what wavelength or intensity of light they used in the study.
Until we have more details and the results have been properly scrutinised, it’s important to view them with caution. In the meantime, other viruses can provide some clues. Research on Sars – a close relative of Covid-19 – found that exposing the virus to UVA for 15 minutes had no impact on how infectious it was. However, the study didn’t look at longer exposures, or UVB, which is known to be more damaging to genetic material.
Then there’s the flu. When scientists analysed hospital admission records in Brazil, they found that the number of flu cases tended to go up during the burning season, when there is more smoke in the atmosphere from forest fires and the UV in sunlight is diluted. Another study found that the longer flu particles were exposed to sunlight for – and the more concentrated it was – the less likely they were to remain infectious. Alas, the study looked at flu suspended in the air, rather than dried onto objects.

“Scientists have found that flu cases in Brazil tend to go up during the burning season, when smoke dilutes UV”
All this means that using sunlight to disinfect surfaces is extremely problematic. First of all, no one knows how long it takes to deactivate Covid-19 with sunlight, or what strength is needed. And even if they did, the amount of UV in sunlight varies depending on the time of day, the weather, the season, and where in the world you live – especially which latitude – so this wouldn’t be a reliable way to kill the virus.”
There’s no money in natural healthcare because you can’t approve what God has already granted. Why because it’s 100% Organic.
Here’s a visual example of Injecting UV light into the body of a patient as a disinfectant to kill viruses and bacteria. pic.twitter.com/BAVkjhVXLK— Kaya Jones (@KayaJones) April 24, 2020
ULTRAVIOLET BLOOD IRRADIATION
http://ubimedical.com/history-of-bt.html
https://infectionscured.com/rise-and-fall-of-ubt
http://drsubi.com/published-studies/viral-studies
https://issels.com/treatment-summary/ultraviolet-blood-irradiation-therapy
https://ncbi.nlm.nih.gov/pmc/articles/PMC6122858
Ultraviolet Irradiation of Blood: “The Cure That Time Forgot”?
by Michael R. Hamblin / 2017
“Ultraviolet blood irradiation (UBI) was extensively used in the 1940s and 1950s to treat many diseases including septicemia, pneumonia, tuberculosis, arthritis, asthma and even poliomyelitis. The early studies were carried out by several physicians in USA and published in the American Journal of Surgery. However with the development of antibiotics, UBI use declined and it has now been called “the cure that time forgot”. Later studies were mostly performed by Russian workers and in other Eastern countries and the modern view in Western countries is that UBI remains highly controversial.
This chapter discusses the potential of UBI as an alternative approach to current methods used to treat infections, as an immune-modulating therapy and as a method for normalizing blood parameters. No resistance of microorganisms to UV irradiation has been reported, and multi- antibiotic resistant strains are as susceptible as their wild-type counterparts.
Low and mild doses of UV kill microorganisms by damaging the DNA, while any DNA damage in host cells can be rapidly repaired by DNA repair enzymes. However the use of UBI to treat septicemia cannot be solely due to UV-mediated killing of bacteria in the blood-stream, as only 5–7% of blood volume needs to be treated with UV to produce the optimum benefit.
https://vimeo.com/232734493
UBI may enhance the phagocytic capacity of various phagocytic cells (neutrophils and dendritic cells), inhibit lymphocytes, and oxidize blood lipids. The oxidative nature of UBI may have mechanisms in common with ozone therapy and other oxygen therapies. There may be some similarities to extracorporeal photopheresis (ECP) using psoralens and UVA irradiation.
https://vimeo.com/231888075
However there are differences between UBI and ECP in that UBI tends to stimulate the immune system, while ECP tends to be immunosuppressive. With the recent emergence of bacteria that are resistant to all known antibiotics, UBI should be more investigated as an alternative approach to infections, and as an immune-modulating therapy.
25.1. Historical Introduction
Ultraviolet (UV) radiation is part of the electromagnetic spectrum with a wavelength range (100–400 nm) shorter than that of visible light (400–700 nm), but longer than x-rays (<100 nm). UV radiation is divided into four distinct spectral areas including vacuum UV (100–200 nm), UVC (200–280 nm), UVB (280–315 nm) and UVA (315–400 nm). Only part of UVB and UVA can reach on earth, because wavelengths shorter than 280 nm are filtered out by the atmosphere especially by the “ozone layer”. In 1801 Johann Wilhelm Ritter, a Polish physicist working at the University of Jena in Germany discovered a form of light beyond the violet end of the spectrum that he called “Chemical Rays” and which later became “Ultraviolet” light [1].

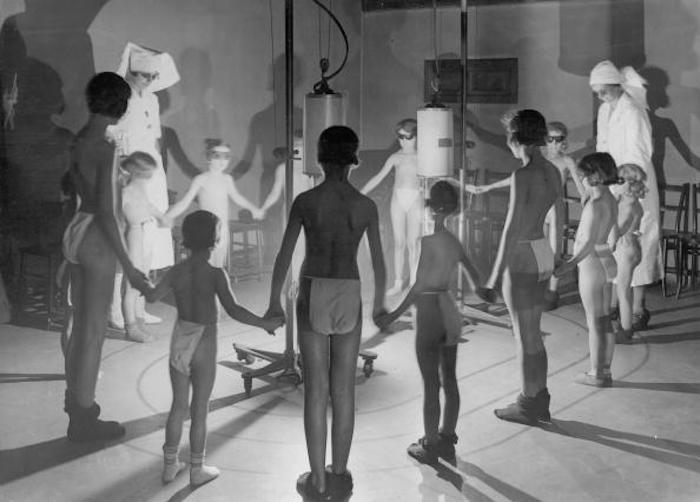
In 1845, Bonnet [2] first reported that sunlight could be used to treat tuberculosis arthritis (a bacterial infection of the joints). In the second half of the nineteenth century, the therapeutic application of sunlight known as heliotherapy gradually became popular. In 1855, Rikli from Switzerland opened a thermal station in Veldes in Slovenia for the provision of helio-therapy [3].

“Children during a light therapy session, 1937”
In 1877, Downes and Blunt discovered by chance that sunlight could kill bacteria [4]. They noted that sugar water placed on a window- sill turned cloudy in the shade but remained clear while in the sun. Upon microscopic examination of the two solutions, they realized that bacteria were growing in the shaded solution but not in the one exposed to sunlight.
The Institution of Radiotherapy, 1934
In 1904, the Danish physician Niels Finsen was awarded the Nobel Prize in Physiology or Medicine for his work on UV treatment of various skin conditions. He had a success rate of 98% in thousands of cases, mostly the form of cutaneous tuberculosis known as lupus vulgaris [5]. Walter H Ude reported a series of 100 cases of erysipelas (a cutaneous infection caused by Streptococcus pyogenes) in the 1920s, with high cure rates using irradiation of the skin with UV light [6].

Emmett K Knott (Fig. 25.1) in Seattle, WA reasoned that the beneficial effects of UV irradiation to the skin obtained by Ude, might (at least partly) be explained by the irradiation of blood circulating in the superficial capillaries of the skin. With his collaborator Edblom, an irradiation chamber was constructed to allow direct exposure of the blood to UV. The irradiation chamber was circular and contained a labyrinthine set of channels that connected the inlet and outlet ports. All these channels were covered with a quartz window that formed the top of the chamber. The irradiation chamber was so designed as to provide maximum turbulence of the blood flowing through (see Fig. 25.2). This was done in order to: (a) prevent the formation of a thin film of blood on the chamber window that would absorb and filter out much of the UV light; (b) insure that all the blood passing through the chamber was equally exposed to UV [7].

Emmett K Knott
Knott and co-workers then carried out a series of experiments using UV irradiation of blood extracted from dogs that had been intravenously infected with Staphylococcus aureus bacteria and hemolytic Streptococcus species, and then the treated blood was reinfused into the dogs. They found that it was unnecessary to deliver a sufficient exposure of UV light to the blood to directory kill all the bacteria in the circulation. It was also found unnecessary to expose the total blood volume in the dogs. The optimum amount of blood to be irradiated was determined to be only 5–7% of the estimated blood volume or approximately 3.5 mL per kg of body weight. Exceeding these limits led to loss of the benefits of the therapy. All the dogs that were treated with the optimized dose of UV to the blood, recovered from an overwhelming infection (while many dogs in the control group died). None of the dogs that were treated and survived, showed any long-term ill effects after 4 months of observation [7].

The Knott Hemo-Irradiator
The first treatment on a human took place in 1928 when a patient was determined to be in a moribund state after a septic abortion complicated by hemolytic streptococcus septicemia. UBI therapy was commenced as a last resort, and the patient responded well to the treatment and made a full recovery [7]. She proceeded to give birth to two children. Hancock and Knott [8] had similar success in another patient suffering from advanced hemolytic streptococcal septicemia. These workers noted that in the majority of cases, a marked cyanosis (blue tinge to the skin caused by a lack of oxygenated blood flow) was present at the time of initiation of UBI.

Sun therapy, 1935
It was noted that during (or immediately following) the treatment a rapid relief of the cyanosis occurred, with improvement in respiration accompanied by a noticeable flushing of the skin, with a distinct loss of pallor. These observations led to application of UBI in patients suffering from pneumonia. In a series of 75 cases in which the diagnoses of pneumonia were confirmed by X-rays, all patients responded well to UBI showing a rapid decrease in temperature, disappearance of cyanosis (often within 3–5 min), cessation of delirium if present, a marked reduction in pulse rate and a rapid resolution of pulmonary consolidation. A shortening of the time of hospitalizations and accelerated convalescence was regularly observed.

“Children listen to a gramophone during sun ray treatment
at the East End Mission in London, 1931”
The knowledge gained in these successful studies led to the redesign of the irradiation chamber to allow a more thoroughly uniform exposure of the circulating blood, and led to the development of the “Knott Technic of Ultraviolet Blood Irradiation.” A number of irradiation units were manufactured and placed in the hands of physicians interested in the procedure, so that more extensive clinical data could be accumulated [7]. The Knott technique involved removing approximately 3.5 mL/kg venous blood, citrating it as an anticoagulant, and passing it through the radiation chamber. The exposure time per given unit of blood was approximately 10 s, at a peak wavelength of 253.7 nm (ultraviolet C) provided by a mercury quartz burner, and the blood was immediately re-perfused [7].
George P Miley at the Hahnemann Hospital, Philadelphia, PA published a series of articles on the use of the procedure in the treatment of thrombophlebitis, staphylococcal septicemia, peritonitis, botulism, poliomyelitis, non-healing wounds, and asthma [9–22]. Henry A Barrett at the Willard Parker Hospital in New York City in 1940 reported on 110 cases including a number of different infections. Twenty-nine different conditions were described as being responsive, including the following: infectious arthritis, septic abortion, osteoarthritis, tuberculosis glands, chronic blepharitis, mastoiditis, uveitis, furunculosis, chronic paranasal sinusitis, acne vulgaris, and secondary anemia [23, 24]. EV Rebbeck at the Shadyside Hospital in Pittsburgh, PA, reported the use of UBI in Escherichia coli septicemia, post-abortion sepsis, puerperal sepsis, peritonitis, and typhoid fever [25–29] and Robert C Olney at the Providence Hospital, Lincoln, NE, treated biliary disease, pelvic cellulitis and viral hepatitis [30–32].
In this chapter, we will discuss the mechanisms and the potential of UBI as an alternative approach to infections and as a new method to modulate the immune system. Our goal is to remind people to continue to do more research and explore more clinical uses. The topics include the efficacy of UBI for infections (both bacterial and viral), to cure autoimmune disease, disease, and the similarities and differences between UBI, and intravenous ozone therapy, and extracorporeal psoralen-mediated photochemotherapy (photophoresis).
25.2. Mechanisms of Action of UBI
One of the major obstacles that UBI has consistently faced throughout the almost 90 years since the first patient was treated has been the lack of understanding of the mechanisms of action. Over the years its acceptance by the broad medical community has been hindered by this uncertainty. Confusion has been caused by the widely held idea that since UV is used for sterilization of water and surgical instruments; therefore its use against infection must also rely on UV-mediated direct destruction of pathogens.
https://www.youtube.com/watch?v=Pr3kuabexV4
Another highly confusing aspect is the wide assortment of diseases, which have been claimed to be successfully treated by UBI. It is often thought that something that appears to be “too good to be true” usually is. UBI affects various functions of red blood cells and various different leukocytes as has been proven in various in vitro studies. A common model is stimulator cells in mixed leukocyte cultures; another is helper cells in mitogen- stimulated cultures. UV also reversed cytokine production and blocked cytokine release. UV can also disturb cell membrane mobilization (Fig. 25.3).

Proposed mechanisms of UBI
25.2.8. Conclusions Regarding Mechanisms
UBI has always caused much confusion, both in the general public and also in some medical professionals, because germicidal UV light (UVC) is used to sterilize water, disinfect surfaces, and as an aid to infection control in operating rooms, and food processing and packaging plants. Many people therefore assume that UBI must act by killing pathogens (bacteria, viruses or other microorganisms) circulating in the bloodstream. However there is no evidence that this is actually the case. Therefore the mechanisms of action must lie in some other action of UV on the various components of blood. Although the entire body of evidence on the mechanisms of action of UBI is very complex, as can be seen from the foregoing material, we can attempt to draw some general conclusions. Firstly UBI is clearly an example of the well-known phenomenon called “hormesis” or “biphasic dose response’.

“Comparison of DNA damage produced by (a) UVB or UVC (intra-strand cross-links), and (b) DNA damage produced by psoralens and UVA (ECP, inter-strand cross-links)”
This phenomenon has been well reviewed by Edward Calabrese from U Mass Amherst [73, 74]. The basic concept states that any toxic chemical substance or drug, or any physical insult (such as ionizing radiation, hyperthermia, or oxidative stress) can be beneficial, protective or even therapeutic, provided the dose is low enough. If the dose is increased, the beneficial or protective effects disappear, and if the dose is even further increased, then the detrimental effects of the treatment become very evident. This is clearly shown by Knott’s original experiments on dogs that led to the establishment of only 5–7% of total blood volume as the optimal amount of blood to be irradiated.
https://www.youtube.com/watch?v=1czxJz4GCuo
UBI appears to have three broadly different classes of effects on different blood components. In the case of neutrophils, monocytes, macrophages, and dendritic cells, UBI can activate phagocytosis, increase the secretion of NO and reactive nitrogen species, and convert the DC phenotype from an immunogenic one into a tolerogenic one, thus perhaps lessening the effects of a “cytokine storm” as is often found in sepsis. In the case of lymphocytes, the effects of UBI are to inhibit (or in fact kill) various classes of lymphocytes. This is not perhaps very surprising, considering the well-established cell-death pathways and apoptotic signaling found in lymphocytes.
However it is not impossible, that the killing of circulating lymphocytes could reduce systemic inflammation, which would again be beneficial in cases of sepsis. It is also clear that UBI can oxidize blood lipids and lipoproteins, and therefore increase oxidative stress. However it is also possible that a brief burst of oxidative stress, may be beneficial, whereas continued chronic levels of oxidative stress have been generally considered as detrimental. Many antioxidant defenses are up-regulated by brief exposure to oxidative stress, and this has been postulated to be one of the fundamental mechanisms responsible for may aspects of hormesis. The oxidative nature of UBI has encouraged us to draw parallels with ozone therapy and other forms of ‘oxygen therapy”.
25.5. Modern Devices to Carry Out UBI
Although it is often said that UBI is “the cure that time forgot” [90, 91], it has not actually been completely forgotten. There are several companies, organizations and devices existing at the present time, which are being used or proposed (on a rather small scale) to carry out UBI, or as it often called “Photoluminescence Therapy (PT)”.
Several websites provide information on UBI and PT. Perhaps one of the most comprehensive is (http://www.mnwelldir.org/docs/uv_light/uv_light3.htm) that provides a listing of practitioners located in USA that offer UBI to patients. UBI medical (http://ubimedical.com/about-us.html) also has a lot of information available. The web-site entitled “Infections cured” (http://infectionscured.com) is also worth checking out. Physicians UBI Awareness Center (http://drsubi.com) even has a video posted online comparing different kinds of UBI machines.
25.6. Conclusion
UV irradiation of blood was hailed as a miracle therapy for treating serious infections in the 1940s and 1950s. In an ironic quirk of fate, this historical time period coincided with the widespread introduction of penicillin antibiotics, which were rapidly found to be an even bigger medical miracle therapy. Moreover another major success of UBI, which was becoming increasingly used to treat polio, was also eclipsed by the introduction of the Salk polio vaccine in 1955 [91]. UBI had originally been an American discovery, but then was transitioned to being more studied in Russia and other eastern countries, which had long concentrated on physical therapies for many diseases, which were more usually treated with drugs in the West.
https://www.youtube.com/watch?v=Z5eV1JcIE1I
However in the last decade the problem of multi-antibiotic resistant bacteria has grown relentlessly. Multidrug-resistant (MDR) and pandrug resistant (PDR) bacterial strains and their related infections are emerging threats to public health throughout the world [92]. These are associated with approximately two-fold higher mortality rates and considerably prolonged hospital admissions [93].
The infections caused by antibiotic resistant strains are often exceptionally hard to treat due to the limited range of therapeutic options [94]. Recently in Feb 2015, the Review on Antimicrobial Resistance stated “Drug- resistant infections could kill an extra 10 million people across the world every year by 2050 if they are not tackled. By this date they could also cost the world around $100 trillion in lost output: more than the size of the current world economy, and roughly equivalent to the world losing the output of the UK economy every year, for 35 years” [95].
Sepsis is an uncontrolled response to infection involving massive cytokine release, widespread inflammation, which leads to blood clots and leaky vessels. Multi-organ failure can follow. Every year, severe sepsis strikes more than a million Americans. It is estimated that between 28–50% percent of these people die. Patients with sepsis are usually treated in hospital intensive care units with broad-spectrum antibiotics, oxygen and intravenous fluids to maintain normal blood oxygen levels and blood pressure. Despite decades of research, no drugs that specifically target the aggressive immune response that characterizes sepsis have been developed.
We would like to propose that UBI be reconsidered and re-investigated as a treatment for systemic infections caused by multi-drug resistant Gram-positive and Gram-negative bacteria in patients who are running out of (or who have already run out) of options. Patients at risk of death from sepsis could also be considered as candidates for UBI. Further research is required into the mechanisms of action of UBI. The present confusion about exactly what is happening during and after the treatment is playing a large role in the controversy about whether UBI could ever be a mainstream medical therapy, or must remain side-lined in the “alternative and complementary” category where it has been allowed to be forgotten for the last 50 years.”
PREVIOUSLY
RADIATION HORMESIS
https://spectrevision.net/2019/06/07/radiation-hormesis/
TUMOR VOLTAGE
https://spectrevision.net/2017/06/08/bioelectric-medicine/
ARCTIC REINDEER SEE in ULTRAVIOLET
https://spectrevision.net/2011/06/03/arctic-reindeer-see-in-ultraviolet/
